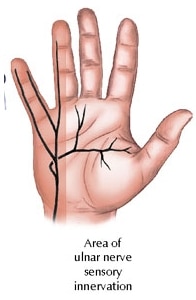
Ulnar tunnel syndrome is an uncommon cause of pain and numbness in the hand. There are three main nerves of the hand; the median nerve, the radial nerve and the ulnar nerve. The ulnar nerve supplies sensation to the 5th finger and one half of the 4th finger. Compression of the ulnar nerve can also cause weakness of the pinch and grip of the hand. The symptoms of ulnar tunnel syndrome include pain, numbness and burning of the 4th and 5th fingers of the hand as well as muscle weakness. Causes of ulnar tunnel syndrome include trauma and fractures or repetitive injury such as in using a jack-hammer or long distance bicycling. Rapid weight gain, rheumatoid arthritis and pregnancy are also associated with this disease. Testing includes X-rays to look for fractures and MRI scans to look for growths or tumors in the wrist. Electromyography (EMG) and Nerve Conduction Studies (NCV) are useful to determine the exact sight of nerve compression and to look for other causes of the symptoms such as a herniated cervical disc or diabetic nerve damage. Treatment begins with conservative modalities such as rest, splinting, physical therapy and medications such as non-steroidal anti-inflammatories. Injection into the area of nerve compression with a local anesthetic and a steroid may decrease the symptoms. In patients who do not respond to conservative treatment, surgery may be indicated to release the nerve entrapment.

